
Analysis of Radio Frequency Identification (RFID) Chip Prevalence in 3 Discrete United States Populations
By John Brugle, Ph.D. on June 8, 2014
John T. Brugle, Ph.D and Mary Franz, Ph.D, M.P.H.
Wyoming Institute of Technology, Human Studies Division
ePUB Ahead of Print
Abstract
Radio Frequency Identification (RFID) Chips have been used extensively in
wildlife ecology and conservation to identify and track individual specimens in
a population. It has been unknown, however, how often RFID chips have been
implanted in human populations for the tracking and identification of
individuals. This study analyzed the prevalence of RFID Chips in 3
geographically discrete populations and found that, on average, 1 in 3
individuals carried an RFID Chip. Interestingly, there was a strong correlation
with RFID Chip presence and previous dental work.
Materials and Methods
Populations
Three discrete human populations, defined by geographic location, were assessed
for the presence of RFID Chips.
Figure 1
Population Midwest (MW) contained 958 individuals from Illinois, Iowa, and
Wisconsin. Population Northeast (NE) contained 987 individuals from Maine, Rhode
Island, and New Jersey. Population South West (SW) contained 1,010 individuals
from Arizona and Nevada. Volunteers were recruited using standard methods and
compensated in a manner consistent with industry standards. All test subjects
were treated in compliance with institutional codes of ethics and standards.
RFID Scanning
Individuals were subjected to full body RFID Chips scanning using previously
detailed protocols. Test subjects were scanned either in the nude or in minimal
undergarments to avoid interference.
Demographic and Personal History Screening
Test subjects provided demographic and personal history, including medical
history, through standard forms. All personal and medical information was coded
in a double blind manner to protect privacy, in compliance with institutional
standards.
Statistical Analysis
Statistical analysis was performed and visualized using R. Significance cut offs
were set at p=0.01. Complete description of the statistical packages used can be
accessed in the supplementary material.
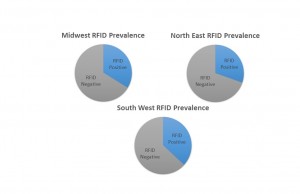
Figure 2
Results
In total, 997 RFID positive individuals were identified out of 2955 individuals
screened. This corresponds to roughly 1 in 3 individuals screened, as shown in
Figure 1. Individual frequency by region can be seen in Figure 2.
Additionally, tooth fillings were identified as the predominant location for
RFID chips. Fifty seven percent of RFID chips identified were located in tooth
fillings. Additional RFID locations and their prevalence can be seen in Figure
3.
.jpg)
Figure 3
Discussion
Our work has shown that approximately 1 in 3 individuals in the United States is
carrying an RFID microchip. Our sample size was sufficiently large (n=2955) and
was spread throughout three distinct geographic regions. Thus, we are
comfortable extrapolating our finding to the broader American population.
Intriguingly, the most frequently identified location for an RFID microchip was
in tooth fillings. This is contrary to popularly held belief that RFID chips are
inserted in the dorsal of the hand near the thumb. More investigation is
required to understand the significance of this finding.